Insights · June 3, 2026
The Prevention Decade.
Why the next era of medicine is defined by healthspan, not just lifespan — and what GLP-1s, epigenetic clocks, and mitochondrial biology actually tell us about aging well.
For most of the last century, medicine measured its success in years of life. We drove down deaths from heart attacks, strokes, and infection, and the average lifespan climbed. That was a genuine triumph. But it produced an uncomfortable second statistic: the gap between how long people live and how long they live well. In the United States, that gap now runs to roughly a decade — ten years, on average, spent managing chronic disease and decline. The defining project of the next decade of medicine is closing it.
Healthspan is a different target than lifespan
Lifespan is when the heart stops. Healthspan is the period during which you are functionally well — mobile, cognitively sharp, metabolically stable, independent. The two are correlated but not identical, and they respond to different interventions. A stent can add years of lifespan after a coronary event; it does very little for the slow erosion of healthspan that precedes it. The shift I find most important is that biology has finally given us tools to measure and move that second number.
The clock is now readable
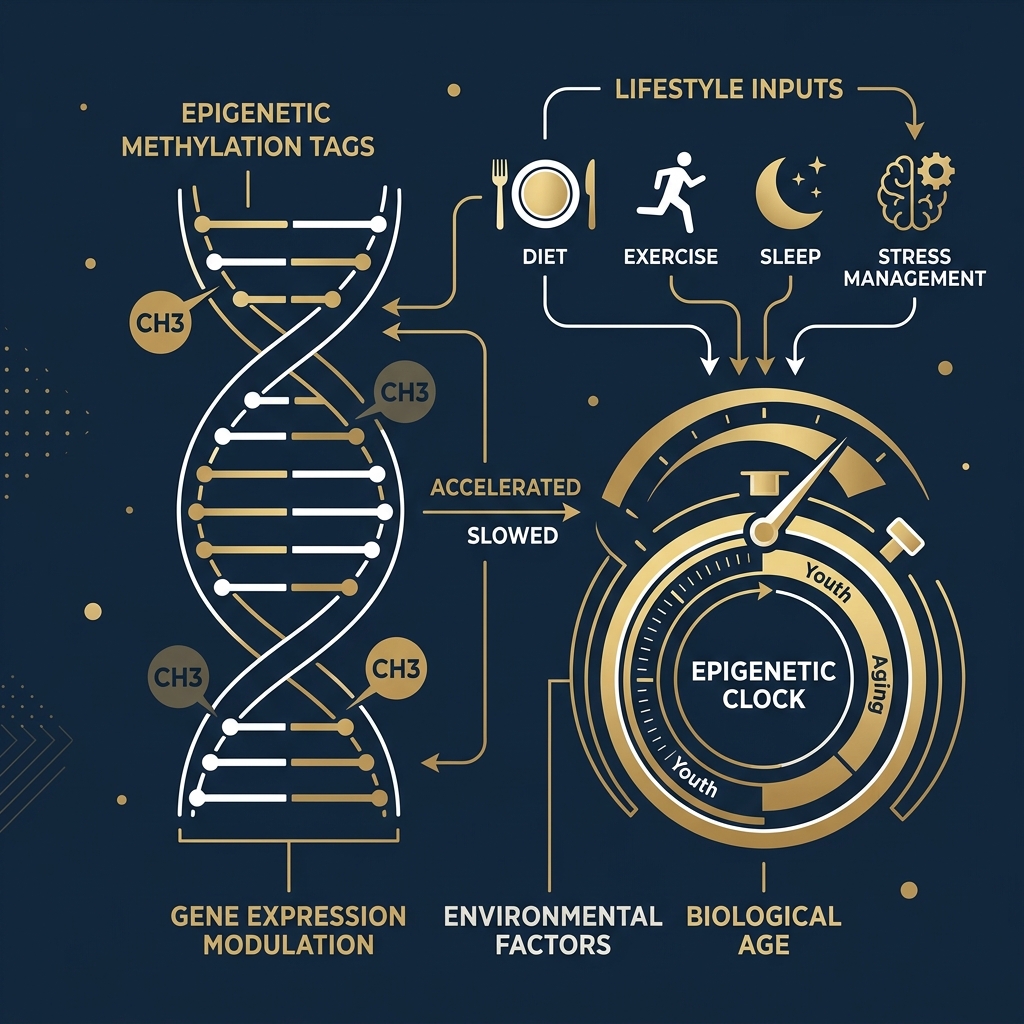
Chronological age — the number on your driver's license — is a poor predictor of how a given body is actually doing. What has changed is that we can now read biological age more directly. Epigenetic clocks, built from patterns of DNA methylation, estimate how much a person's tissues have actually aged. Two people born the same year can differ substantially on these measures, and the difference tracks with real outcomes: cardiovascular events, cognitive decline, mortality.
That matters because a readable clock is, in principle, a movable clock. If you can quantify biological age, you can ask whether an intervention — exercise, a drug, a change in metabolic state — actually slows it, instead of guessing. Much of my own research at Michigan has lived at this intersection, linking cardiorespiratory fitness, multi-omic biomarkers, and mitochondrial biology to the trajectory of aging. (More on that work is on the research page.)
Why mitochondria keep showing up
If there is a unifying thread running through cardiovascular aging, it is the mitochondrion. Reactive oxygen species damage mitochondrial DNA; that damage releases molecular danger signals; those signals drive the low-grade chronic inflammation we now call inflammaging; and inflammaging accelerates nearly every age-related disease, from atherosclerosis to neurodegeneration. It is a vicious cycle, and it is also a target. Interventions that protect mitochondrial function — including the most ordinary one, regular aerobic exercise — may do more for healthspan than most of what we can currently prescribe.
The GLP-1 moment, in context
No discussion of prevention today is complete without the GLP-1 receptor agonists. Drugs originally developed for diabetes are now reshaping how we treat obesity, and the cardiovascular outcome data are genuinely striking. But the right way to read them is not as a weight-loss story. It is a metabolic-aging story: these agents appear to act on exactly the inflammatory and cardiometabolic pathways that erode healthspan. The open questions — durability, cost, equity of access, what happens when people stop — are the questions that will decide whether this becomes a prevention tool or a luxury one. I write about that tension at length in The Great Healthcare Disruption, and in more depth on the GLP-1s & cardiometabolic topic page.
What this means for the next ten years
Put these threads together and a picture emerges. We are moving from a medicine that waits for disease to a medicine that measures and protects healthspan — with biological-age readouts, mitochondrial and metabolic targets, and a new class of drugs that, used wisely, fit that frame. The hard part will not be the science. It will be the system: who gets access, who pays, and whether we deploy these tools to compress the decade of decline for everyone or only for those who can afford it.
That is the question worth spending the next decade on. It is also, not coincidentally, the question I keep returning to in my writing and my work at Michigan.
More like this.
New essays on prevention, longevity, and the business of medicine — occasional, never spam.